Which Medical Plan is Right?
Liberty Health offers employees a choice of four (4) medical plans through Blue Cross Blue Shield of North Carolina. The HPN plan is only available for employees who live or work in these markets: RTP, Triad, Charlotte, Hickory/Statesville, Miami, Memphis.
You are eligible to enroll in the medical plan after the first of the month following 30 days of full-time employment. Eligible dependents include your spouse and your dependent children through the end of the month in which they turn 26.
The following chart is a high-level overview of coverage. Please refer to actual plan documents or contact BCBS of NC customer service at 1.800.517.8072 for benefit verification.
Medical Plan Comparison
Basic, Standard, Premium Plans
| Basic | Standard | Premium | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Benefit Highlights | In-Network | Out of Network | In-Network | Out of Network | In-Network | Out of Network | |||||
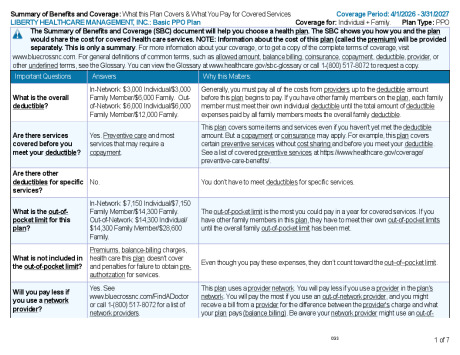
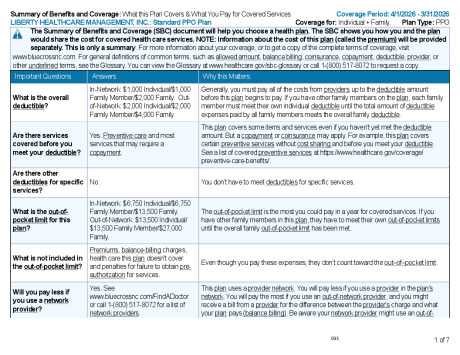
| Deductible | Individual | $3,000 | $6,000 | $1,000 | $2,000 | $500 | $1,000 | ||||
| Family | $6,000 | $12,000 | $2,000 | $4,000 | $1,000 | $2,000 | |||||
| Deductible Timing | Plan Year | Plan Year | Plan Year | ||||||||
| Deductible Basis | Embedded | Embedded | Embedded | ||||||||
| Deductible & Copays Included in OOP Max | Yes | Yes | Yes | ||||||||
| Coinsurance | 30% | 50% | 20% | 40% | 20% | 40% | |||||
| Max Out of Pocket | Individual | $7,150 | $14,300 | $6,750 | $13,500 | $6,350 | $12,700 | ||||
| Family | $14,300 | $28,600 | $13,500 | $27,000 | $12,700 | $25,400 | |||||
| Hospital | 30% after Deductible | 50% after Deductible | 20% after Deductible | 40% after Deductible | 20% after Deductible | 40% after Deductible | |||||
| Outpatient | 30% after Deductible | 50% after Deductible | 20% after Deductible | 40% after Deductible | 20% after Deductible | 40% after Deductible | |||||
| Office Visits | PCP | $30 Copay | 50% after Deductible | $25 Copay | 40% after Deductible | $15 Copay | 40% after Deductible | ||||
| Specialist | $60 Copay | 50% after Deductible | $50 Copay | 40% after Deductible | $40 Copay | 40% after Deductible | |||||
| Preventive Care | 100% Covered per ACA Guidelines | 50% after Deductible | 100% Covered per ACA Guidelines | 40% after Deductible | 100% Covered | 40% after Deductible | |||||
| Teladoc | $0 Acute Care/Behavioral Health $60 Dermatology | Not Covered | $0 Acute Care/Behavioral Health $50 Dermatology | Not Covered | $0 Acute Care/Behavioral Health $40 Dermatology | Not Covered | |||||
| Chiropractic Care | 30% after Deductible 30 visit limit per benefit period | 50% after Deductible 30 visit limit per benefit period | 20% after Deductible 30 visit limit per benefit period | 40% after Deductible 30 visit limit per benefit period | 20% after Deductible 30 visit limit per benefit period | 40% after Deductible 30 visit limit per benefit period | |||||
| Routine Vision Exam | 100% Covered | Not Covered | 100% Covered | Not Covered | 100% Covered | Not Covered | |||||
| Cologuard | 100% Covered | 100% Covered | 100% Covered | ||||||||
| Prescription | Retail- 30 day supply NetResults 5 tier | Tiers 1 & 2: $10 Tiers 3, 4 & 5: 100% to $125 |
Tiers 1 & 2: $10 Tiers 3, 4 & 5: 50% to $100, Min $50 |
Tiers 1 & 2: $10 Tier 3: $30 Tiers 4 & 5: 25% to $100, Min $50 |
|||||||
| Mail Order (McNeill's Pharmacy) - 31 to 90 day supply - only option for mail order | Tiers 1 & 2: $0 Tiers 3, 4 & 5: 100% to $125 |
Tiers 1 & 2: $0 Tiers 3, 4 & 5: 50% to $100, Min $50 |
Tiers 1 & 2: $0 Tier 3: $30 Tiers 4 & 5: 25% to $100, Min $50 |
||||||||
| Formulary | NetResults 5 tier restricted formulary | NetResults 5 tier restricted formulary | NetResults 5 tier restricted formulary | ||||||||
| Emergency Care | ER Copay | $500 Copay | $350 Copay | $250 Copay | |||||||
| Urgent Care | $50 Copay | $40 Copay | $30 Copay | ||||||||
| Nutritional Counseling | 100% Covered Unlimited Visits | 50% after Deductible Unlimited Visits | 100% Covered Unlimited Visits | 40% after Deductible Unlimited Visits | 100% Covered Unlimited Visits | 40% after Deductible Unlimited Visits | |||||
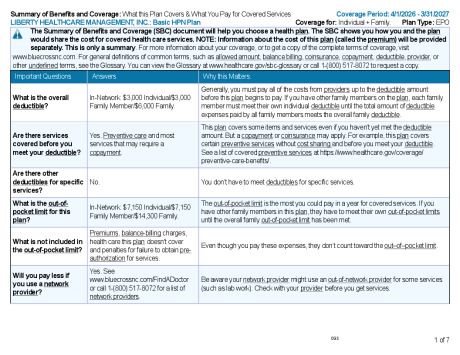
HPN Plan
Only Available for employees who live or work in these markets: RTP, Triad, Charlotte, Hickory/Statesville, Miami, Memphis
| HPN In-Network Coverage Only | |||
|---|---|---|---|
| Benefit Highlights | In-Network | ||
| Deductible | Individual | $3,000 | |
| Family | $6,000 | ||
| Deductible Timing | Plan Year | ||
| Deductible Basis | Embedded | ||
| Deductible & Copays Included in OOP Max | Yes | ||
| Coinsurance | 30% | ||
| Max Out of Pocket | Individual | $7,150 | |
| Family | $14,300 | ||
| Hospital | 30% after Deductible | ||
| Outpatient | 30% after Deductible | ||
| Office Visits | PCP | $30 Copay | |
| Specialist | $60 Copay | ||
| Preventive Care | 100% Covered per ACA Guidelines | ||
| Teladoc | $0 Acute Care/Behavioral Health $60 Dermatology | ||
| Chiropractic Care | 30% after Deductible 30 visit limit per benefit period | ||
| Routine Vision Exam | 100% Covered | ||
| Cologuard | 100% Covered | ||
| Prescription | Retail- 30 day supply NetResults 5 tier | Tiers 1 & 2: $10 Tiers 3, 4 & 5: 100% to $125 | |
| Mail Order (McNeill's Pharmacy) - 31 to 90 day supply - only option for mail order | Tiers 1 & 2: $0 Tiers 3, 4 & 5: 100% to $125 | ||
| Formulary | NetResults 5 tier restricted formulary | ||
| Emergency Care | ER Copay | $500 Copay | |
| Urgent Care | $50 Copay | ||
| Nutritional Counseling | 100% Covered Unlimited Visits | ||

Blue Connect

Blue Connect Mobile

Blue Connect How to Register Guide

Blue Connect Details

ID Card

Get the Most of Your Plan
LIBERTY HEALTHCARE MANAGEMENT INC._SBC_Basic PPO Plan_04012026
LIBERTY HEALTHCARE MANAGEMENT INC._SBC_Standard PPO Plan_040120206
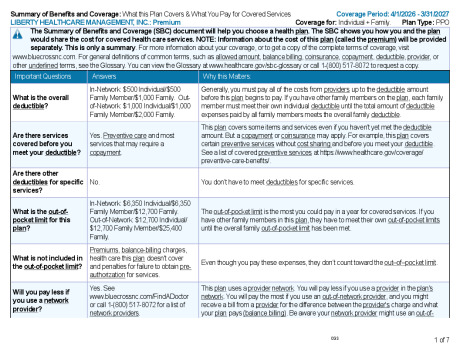
LIBERTY HEALTHCARE MANAGEMENT INC._SBC_Premium_04012026